Prehab: The Boring Routine That Keeps You on the Start Line
I hurt my back backcountry skiing. Not a dramatic fall or a helicopter rescue. Just one too many days of heavy powder turns without the core strength to absorb them. My lower back seized up and didn't let go for weeks.
A couple of years later, I tore my SLAP in my shoulder swimming. Too much volume, not enough maintenance work on the rotator cuff. A cortisone shot got me past the acute pain, but the message was clear: the injury didn't come from one bad stroke. It came from hundreds of sessions without the supporting work that would have kept the joint healthy.
Both times, the fix wasn't complicated. And both times, the prevention would have been even simpler.
What prehab actually is
Prehab is preventative exercise targeted at the joints and tissues most likely to fail under training load. It's not physical therapy (that's what happens after something breaks). It's not stretching (though some of it involves flexibility work). It's a short, specific routine designed to address the vulnerabilities your sport creates before they become injuries.
For my back, that means Pallof presses, bridges, single-leg bridges, hip internal rotation, thoracic rotation, pelvic tilts, and hip extensions. For my shoulder, it's prone trap raises, chest-supported rows, side-lying external rotation with a slow eccentric, and dead hangs.
Neither routine takes more than twenty minutes. Neither is impressive to watch. That's rather the point.
Ten ways active people over 50 get hurt
After building TheNextHill and talking to hundreds of athletes in this age group, the same injuries come up over and over. Here are the ten most common, and every one of them is preventable with the right prehab.
1. Achilles tendinopathy. The tendon stiffens with age as it loses water content and elasticity. Running and hiking volume is the usual trigger. Eccentric heel drops, the gold standard since Alfredson's 1998 study, take a few minutes a day. The tendinopathy they prevent takes three to six months to resolve.
2. Plantar fasciitis. The fascia under your foot loses its spring after 50. Runners and trekkers are the most common victims. Toe curls, calf stretches, and balance work on an unstable surface keep it healthy. Ignoring it means months of hobbling out of bed every morning.
3. Knee osteoarthritis and meniscal stress. The most common complaint in trekkers, skiers, and cyclists over 50. The cartilage thins. The meniscus frays. But targeted quad strengthening (terminal knee extensions, wall sits, step-downs) reduces load on the joint surfaces and keeps you moving.
4. Rotator cuff impingement and tears. The rotator cuff degenerates with age whether you train or not. Swimming, climbing, and overhead movements accelerate it. Band external rotations, scapular wall slides, and face pulls take ten minutes and keep the shoulder functioning. Rotator cuff surgery takes four to six months of recovery.
5. Lower back pain and disc issues. Sustained lumbar flexion on the bike, heavy pack carry on treks, and age-related disc dehydration make this the single most common complaint in the 50+ adventure athlete. I know this one personally. Core stabilization work keeps you out of trouble.
6. IT band syndrome. That sharp pain on the outside of the knee that shows up at mile 8 of every run. Weak glutes are almost always the root cause. Side-lying hip abduction, clamshells with a mini-band, and monster walks fix the weakness that causes it. Foam rolling the IT band itself is treating the symptom, not the problem.
7. Hamstring strains and tears. The muscle that gives out when you increase speed work too fast. After 50, the hamstring loses elasticity and takes longer to recover between hard sessions. Nordic curls and single-leg Romanian deadlifts build the eccentric strength that prevents the tear.
8. Blisters. The number one medical reason people abandon multi-day treks like the Camino de Santiago. A 2016 study in Wilderness & Environmental Medicine found blisters affected 74% of participants in multi-stage endurance events. Skin thins after 50, reducing its resistance to shearing forces. The fix is progressive loaded walks in your actual trek footwear, intrinsic foot strengthening (toe yoga, towel scrunches), and barefoot walking to build protective calluses. If your feet haven't done the distance in the actual gear, blisters on day three are almost guaranteed.
9. Ankle sprains and fractures. Proprioception, your ability to sense joint position, declines measurably with age. The ankle rolls more easily on uneven terrain and recovers more slowly. Trail runners, trekkers, and skiers are the most exposed. Single-leg balance progressions restore what the body is losing.
10. Stress fractures. Bone density drops after 50, especially in women. High-mileage runners and trekkers are most at risk. Controlled impact loading (hopping drills, calf raises) stimulates bone remodeling. A stress fracture means six to twelve weeks of zero impact activity.
Every one of these injuries follows the same pattern: progressive tissue deterioration that training volume exposes. And every one of them responds to a targeted prehab routine that takes less time than warming up.
The real cost of skipping it
When I talk to people over 50 who've stopped training, the reason is almost never "I lost motivation." It's "I got hurt." These injuries don't come from one bad session. They come from hundreds of sessions without the maintenance work that would have kept the tissue healthy.
I know because I've been that person. Twice. My back and my shoulder both told me the same thing: you can't just train the engine and ignore the chassis.
The hard part is doing the boring thing consistently when nothing hurts yet.
How we built it into TheNextHill
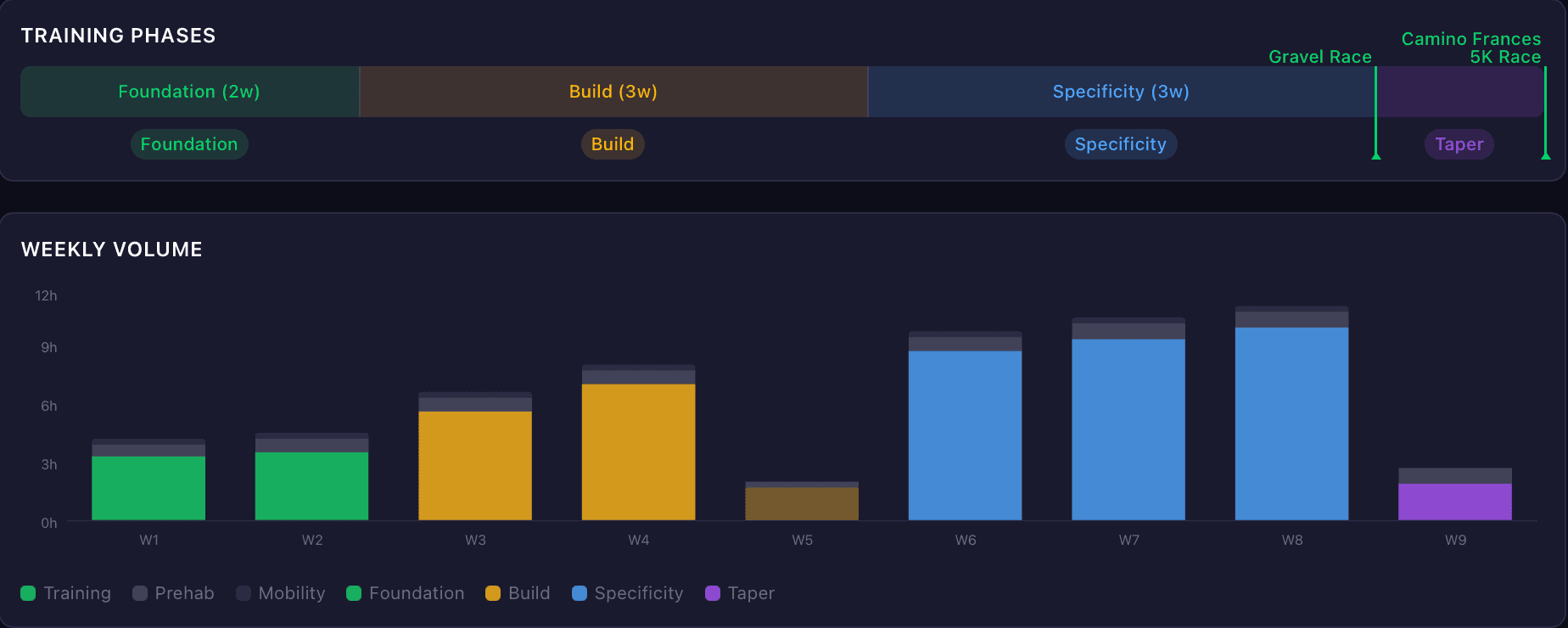
Every training plan TheNextHill generates includes prehab by default. Not as an afterthought. As a first-class part of your training week. The system maps your adventure type to the injuries most likely to sideline you, suggests exercises from a curated library of fifty evidence-based exercises across those ten injury categories, and puts them on your calendar.
Training for a trek? It flags knee osteoarthritis, plantar fasciitis, and ankle sprains. Training for a triathlon? Rotator cuff, lower back, and Achilles tendinopathy. Training for a cycling event? Lower back, knee, and hip flexor.
You can customize the routine, add exercises, remove ones that don't apply. If you've had a specific injury before, you can add targeted work for it. The goal is a personal routine you'll actually do, not a forty-minute session you'll skip.
Because the best prehab routine is the one you do on Tuesday when your shoulder feels fine and there's no obvious reason to bother. That's the whole point. By the time there's an obvious reason, you're already booking the cortisone shot.
I learned that the hard way. Twice. You don't have to.
Found this useful? Share it.